The priorities of women’s mental health organisations globally
Celebrating International Women’s Day 2026
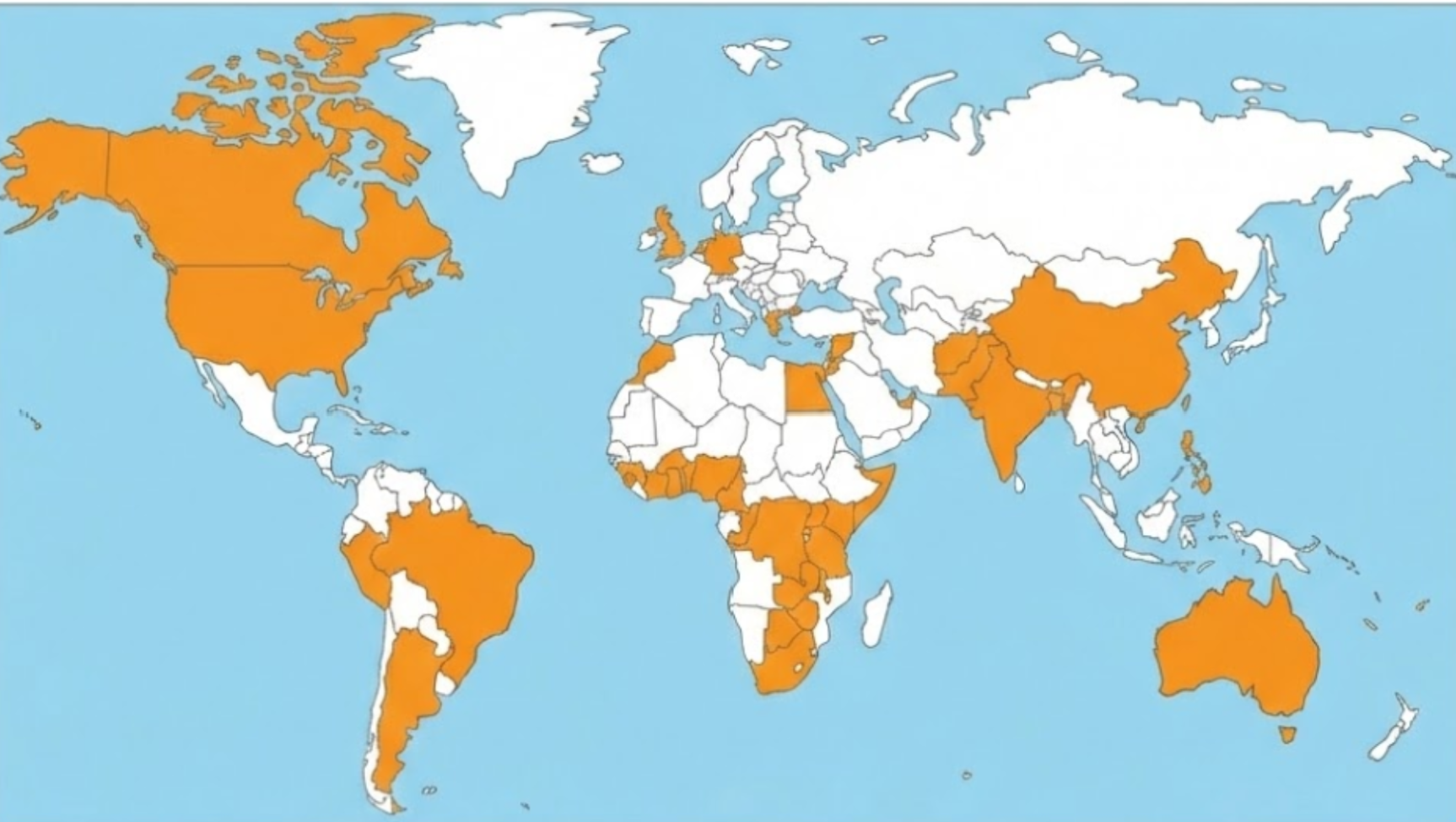
Across our Global Mental Health Action Network’s global and growing membership there are several civil society organisations that focus on women’s mental health. On our last outreach, over 100 organisations in 39 countries have engaged directly with our work. It remains critical that their voices continue to shape the field. We are presenting here their advocacy priorities and key areas for their work.
Top Policy and System Change priorities advocated for by women’s mental health organisations
GMHAN members outline what, in their view (and in their own context), are the two most important policy and system changes that need to happen in their country (or region) over the next three years to improve mental health for all.
1. Full Integration of mental health into Primary Healthcare (PHC) and Community Systems
The most widely cited challenge from women’s mental health organisations is the current healthcare system's reliance on centralised, specialist hospitals, making mental health services inaccessible, expensive, and stigmatised.
Goal: To decentralise care by formally integrating mental health screening, basic psychosocial support, and referral pathways into Primary Healthcare (PHC) - inclusive of maternal health services - as well as utilising non-traditional spaces like schools, faith-based groups, and women's groups.
Mechanism: This includes implementing task-sharing policies to train general practitioners, nurses, midwives and community health workers in basic mental health care.

2. Multisectoral Approach / Mental Health in All Policies
Women’s health organisations emphasise that mental health is a cross-cutting issue driven by poverty, violence, and inequality, meaning its solutions cannot be siloed within the Ministries of Health alone.
Goal: To establish policy frameworks that legally mandate other sectors to allocate budgets and coordinate efforts toward mental health outcomes.
Key Sectors: The most commonly cited sectors for required integration include Social Protection (e.g. linking cash transfers to mental health outcomes), Gender-Based Violence response (e.g. mandating trauma-informed care in safe houses), Education (e.g. compulsory mental health literacy), and Law Enforcement (e.g. anti-stigma training and diversion from the criminal justice system).
3. Prioritising Prevention, Promotion, and Stigma Reduction
A significant number of women’s mental health organisations focus on upstream interventions to prevent mental health crises and tackle the stigma that is often a greater barrier to care than cost.
Goal: To shift policy away from a reactive, crisis-management model toward preventative care and wellbeing.
Mechanism: This includes national anti-stigma campaigns, integrating mental health literacy into school curricula, and funding structured community-based preventative structures like peer support circles and safe spaces.
4. Dedicated and Locally-Driven Funding
Women’s health organisations highlight that policy progress is limited without committed and appropriate financing.
Goal: To move beyond simply having a policy and ensure there is dedicated, sustained, and traceable funding at both national and sub-national levels.
Context-Specific Investment: There is a call for funding strategies to be co-designed with local actors to ensure investments reflect community needs rather than priorities driven by the Global North.
5. Formalising Peer-Led and Gender-Responsive Services
A specific and recurring theme for women’s mental health organisations, particularly in the context of key populations, is the need to formally recognise and integrate non-clinical, lived experience expertise.
Peer-Led Care: Several responses call for a national policy to formally recognise, certify, and directly fund peer supporters and community health workers from key populations (e.g., people who use drugs, sex workers) as an accredited part of the health workforce.
Gender-Responsiveness: Policy changes are requested to establish gender-responsive protocols (e.g. trauma-informed care pathways for GBV survivors, mental health support integrated into maternal and adolescent health services) to address the distinct mental health needs of women and girls.
Top drivers of poor mental health and suffering currently, according to women’s mental health organisations
GMHAN members outline what, in their view (and in their own context), are the two biggest drivers of poor mental health and suffering that should be prioritised for policy action over the next three years.

1. Systemic Stigma, Criminalisation, and Low Mental Health Literacy
This is the most cited driver by women’s mental health organisations, which creates a paralysing climate of fear, driving people away from seeking help.
It includes broad socio-cultural stigma around mental illness, sexism and gender-based discrimination, widespread low mental health literacy, and specifically, the criminalisation of poverty and survival (e.g. drug use and sex work), which actively inflicts trauma and suffering, most commonly on women.
2. Poverty and Economic Insecurity
Women’s mental health organisations consistently view financial stress as a central, chronic driver of poor mental health.
Key drivers encompass unemployment, rising costs of living, financial precarity, and the lack of social safety nets, which leads to sustained anxiety, depression, and feelings of hopelessness. The concept of "gendered poverty" is highlighted, where women carry disproportionate burdens of caregiving alongside economic responsibilities.
3. Violence, Trauma, and Harmful Gender Norms
Violence carries acute and chronic mental health consequences.
It includes Gender-Based Violence (GBV), domestic violence, and the trauma resulting from armed conflict, displacement, and harmful cultural practices (e.g. child marriage), which are cited as major precipitants of mental health crises like PTSD and depression.
4. Inadequate System Funding and Political Prioritisation
This addresses the governmental and institutional failure to allocate sufficient resources to women’s mental health.
It includes the lack of political will to make gender-sensitive mental health a priority, insufficient budget allocation, and the resulting shortage of trained mental health professionals and accessible services.
Biggest protective factors for good mental health and wellbeing that should be prioritised, according to women’s mental health organisations
GMHAN members outline what, in their view (and in their own context), are the two biggest protective factors for good mental health and wellbeing that should be prioritised to be made more widely accessible and available for everyone over the next three years.
1. Economic Empowerment and Social Protection
This is the most frequently cited protective factor by women’s mental health organisations, directly addressing the core driver of poverty and economic insecurity identified earlier.
It includes the need for policies that provide dignified livelihoods, job security, and financial independence, and expand social safety nets (like cash transfer programs) to mitigate the chronic stress of poverty.
2. Strong Social and Community Support
Women’s mental health advocates emphasise the critical role of social connection, family bonds, and a sense of belonging in building resilience.
This includes formalising and funding peer support networks and community-based structures (e.g. safe spaces, women's groups, faith-based organizations) that can offer non-judgmental, immediate emotional support.
3. Mental Health Literacy and Stigma-Free Environments
This factor is viewed as essential for reducing the stigma that prevents help-seeking, particularly for women.
It involves implementing policies to increase mental health literacy through public education, school curricula, and media reform, thereby creating a stigma-free environment where women feel safe to speak about their struggles and access care without fear of discrimination or criminalization.
4. Access to Integrated, Quality Healthcare
Access to good healthcare remains a foundational protective factor for women’s mental health.
This refers to the need for affordable, accessible, and high-quality mental health services that are fully integrated into the Primary Healthcare (PHC) system.

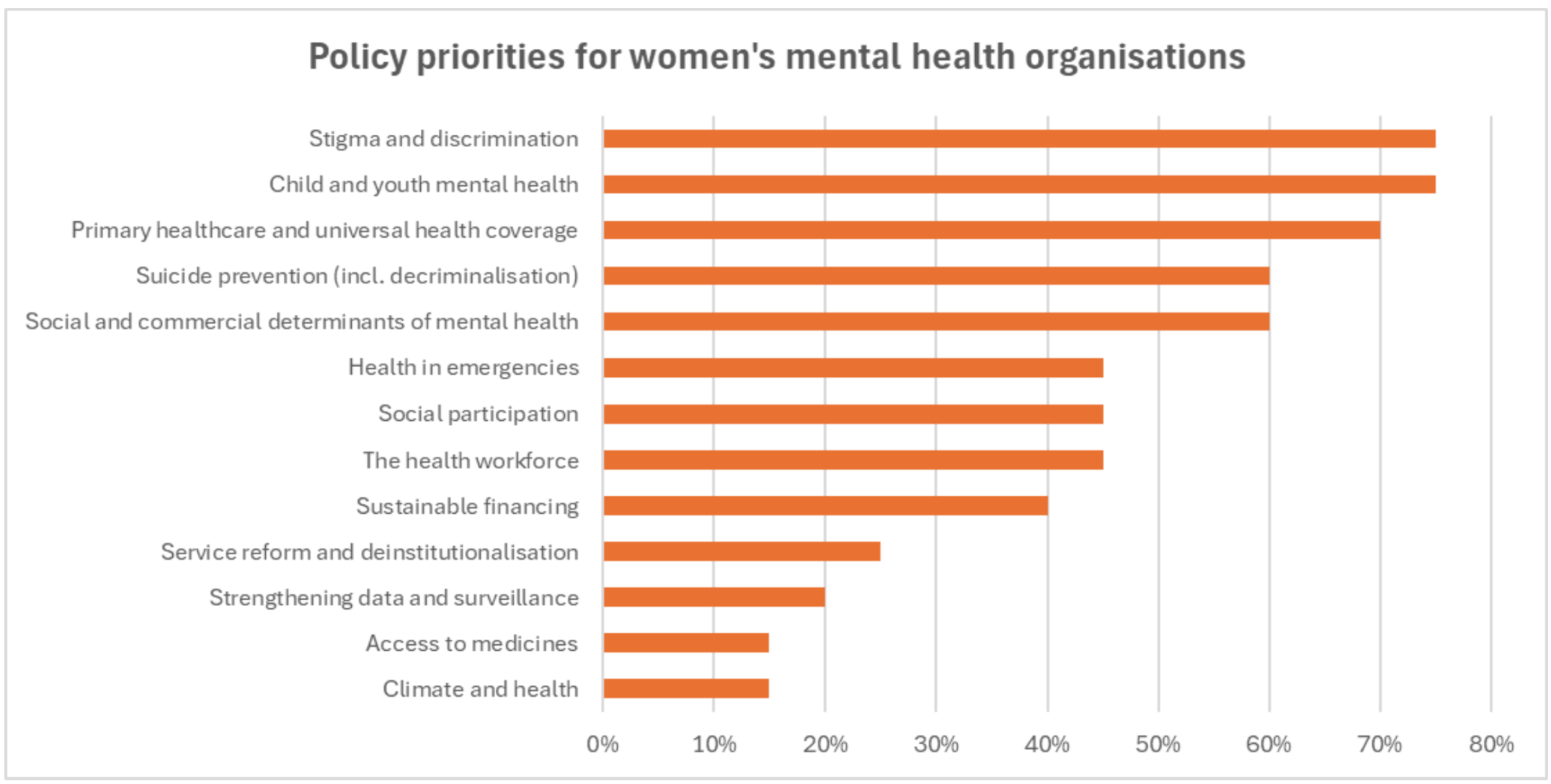
Global priorities for mental health advocacy for women’s mental health organisations
Over the past 2 years, and especially in the lead up to the United Nations High-Level Meeting on Non-Communicable Diseases and Mental Health, our global community has been prioritising the below areas for policy influencing. The chart below shows which of these are also priorities in the advocacy work of women’s mental health organisations that are members of GMHAN.
GMHAN Member Stories from across Africa for International Women’s Day
Access inspiring and learning member stories from across the membership of the Global Mental Health Action Network.
Naomi Dick Kaba - Hakili Nafaya Institute, Côte d'Ivoire
“What I would share with the global community is this: advocacy must be systemic, collective, and rooted in lived experience. When policy reform, regional solidarity, and community storytelling intersect, mental health becomes a social movement.”
Sia Edward - East African Community Mental Health Network, Tanzania
“Challenge stigma, but also challenge systems that exclude mental health from financing and policy priorities. And most importantly, remember that culture matters. Mental health must be grounded in the realities of communities while connected to global solidarity.”
Maxwell Chacha - Valid Dream Mentorship, Kenya
“My journey into mental health advocacy began not in a classroom or conference hall, but on the streets, sitting with young women injecting heroin behind a market. I asked no questions about their past. I simply stayed. Over weeks, they began to speak—not about addiction, but about childhood violence, lost children, police brutality, and the profound exhaustion of being hunted simply for surviving. I learned that their mental distress was not pathology. It was a legitimate response to an illegitimate system.”
Esta Richard Etim - Smart-Fit Trybe, Nigeria
“One of the most important things I have learned is that mental health is deeply connected to daily life. In Nigeria, many women carry economic pressure, caregiving responsibilities, and strong cultural expectations, often without emotional support. These realities must be acknowledged in policy and programming.”
Akekelwa Catherine Chitonka - RefuCare Initiative, Zambia
“In 2023, I co-founded RefuCare Zambia because I was tired of working around broken systems - I wanted to build alternatives. Today, RefuCare serves over 500 adolescent girls and young women whom Zambia's health system has completely abandoned: girls with albinism facing violence and educational exclusion, child marriage survivors denied reintegration support, refugee women in remote settlements, and rural adolescents with zero access to mental health care.”
Anne-Sharlene Murapa - Kurapa Moyo, South Africa
“I founded Kurapa Moyo from that place of inquiry. My work focuses particularly on women because I lead from the lens of an African woman, and I believe our experiences deserve intentional centring. My focus on the continent does not mean I limit my learning to it. I engage globally, but I interpret and apply what I learn through local realities.”



